Single Payer Health Care






What is Single Payer Health Care?
Single payer health care is a health care system where a “single” fund pays for health care costs (rather than private insurers).
There are many different ways single payer can work, but the general idea is 1. to create a universal healthcare system (a system that covers everyone) where, 2. at least basic coverage is handled by a single fund (hybrid systems can use a mix of private and public insurance).
Below we discuss everything single payer and answer many common questions about single payer healthcare.
Defining Single Payer Health Care
In terms of healthcare, the term “single payer” describes the funding mechanism (health care financed by a single public body from a single fund).
Single payer does not specify the type of delivery, or for whom doctors work.
Given this, there are many different types of single payer systems throughout the world that employ unique tactics in terms of insurance, delivery of services, and funding (to differing degrees of success).
Some systems like Britain’s NIH use a fully public system, some like Australia’s Medicare use a mix of private and public funding and delivery methods.
Thus, some of these systems look a lot like the mix of private and public systems we find in America’s “Medicare” and “ObamaCare,” while others are fully “government run” like America’s VA.
Here you should note that while America has a few healthcare programs that are essentially single payer systems, like Medicaid, VA, and Medicare for example, America doesn’t have universal coverage (AKA healthcare-for-all) because the current system excludes tens of millions based on cost and other factors.
The public option is like single payer, but includes a single fund all citizens can buy into (they can “opt” into).
Below we explain single payer, one type of universal healthcare system solution.
With that in mind, we’ll also explain all-payer, the public option, Medicare-for-all, the mandate system, and different ways universal healthcare systems like single payer can work.
Start, let’s look at some quick facts about single payer, how it works, and how it is different from other universal healthcare solutions.
The United States is the Only Highly Developed Country Without Universal HealthCare (not Single Payer)
Sometimes people say the the U.S. is the only major country without “single payer,” but that isn’t exactly right. It is the only one with universal healthcare (some universal systems are single payer systems, but not all are).
With that said, of the top 51 countries with “very high” human development according to the Human Development Index[1], the United States is the only country without some form of a Universal HealthCare system [with the note that a few countries are in the process of implementing their universal systems and some are notably working better than others].”
The list of “highly developed” countries with Universal HealthCare includes: 1 Norway 2 Australia 2 Switzerland 4 Germany 5 Denmark 5 Singapore 7 Netherlands 8 Ireland 9 Iceland 10 Canada 10 United States 12 Hong Kong 13 New Zealand 14 Sweden 15 Liechtenstein 16 United Kingdom 17 Japan 18 South Korea 19 Israel 20 Luxembourg 21 France 22 Belgium 23 Finland 24 Austria 25 Slovenia 26 Italy 27 Spain 28 Czech Republic 29 Greece 30 Brunei 30 Estonia 32 Andorra 33 Cyprus 33 Malta 33 Qatar 36 Poland 37 Lithuania 38 Chile 39 Saudi Arabia 40 Slovakia 41 Portugal 42 United Arab Emirates 43 Hungary 44 Latvia 45 Argentina 45 Croatia 47 Bahrain 48 Montenegro 49 Russia 50 Romania 51 Kuwait.
TIP: To be clear, this doesn’t mean that every one of these systems delivers the quality of care the U.S. does, and this doesn’t mean everyone of these systems is “working perfectly,” it simply means those countries all have some form of universal healthcare. Sometimes people will cite the first 33 countries on the list to avoid having to go into details, but the reality is the list keeps going for a while until you find a developed country that has an uninsured rate as high as the U.S. (and this is before the ACA repeal and replace bill!)
SEE: U.S. is the Only Developed Country that Doesn’t Have Universal HealthCare.
TIP: The United States was on its way to universal healthcare with the Affordable Care Act (ObamaCare) and its “mandate,” subsidies, and Medicaid expansion, as some universal systems are mandate-based. However, too many factors kept the uninsured rate high even under the ACA. For example, states refused to expand Medicaid. As a result, the US still hasn’t made the list of developed countries with universal healthcare, and this is only more true here in 2017 now that the mandate is facing repeal and the BCRA (the ACA repeal and replace bill) seeks to cut Medicaid funding and assistance.
Quick Facts About Single Payer
With the main points covered, below are some quick facts about single payer to help you understand the general conversation surrounding single payer and universal healthcare.
- Many countries have universal healthcare systems, many but not all also have single payer systems (or a hybrid single payer system). See a List of countries with universal health care and a list of countries with a Single-payer healthcare system or a hybrid.
- The “single payer” part refers to funding, not delivery.
- A single payer fund can have a private healthcare delivery system, a public delivery system, or a mix of the two.
- A fund can be controlled by any agency, private or public. Although the fund is typically organized and overseen by the government, it doesn’t have to be.
- A single payer system can also allow for supplemental coverage (like Medicare does; Medicare is essentially a single payer universal healthcare system… for seniors only).
- If a country also uses private coverage, it is a “hybrid system.” Almost every country with single payer has a hybrid system.
- People often use the term “single payer” to refer to universal healthcare (and likewise the term Medicare-for-all gets used as a synonym too).
- Universal healthcare is any system that seeks to provide at least access to care for all, even if there is supplemental coverage, mandates, private coverage, or market based approaches.
- ObamaCare would have counted as universal healthcare (or at least come close) if it had not excluded our poorest (by state rejecting the expansion of Medicaid).
- In the United States, our current Medicare system is a single payer system. If we expanded that to every citizen it would be “Medicare-for-All” (like the bill Bernie has been promoting). See Bernie’s Bill or Australia’s Medicare for all system. Likewise Medicaid, for those who qualify, in states that expanded, is a quasi-universal system.
- If everyone had access to care, like those with Medicare and Medicaid (in states that expanded) do, we would therefore have “a universal healthcare system” in the United States of America.
- Today, not only are we not moving toward single payer, a public option, or universal coverage, via TrumpCare… we are actually moving further away from it by getting rid of the mandate system and Medicaid expansion. The last TrumpCare bill was projected to leave 52 million of our 320 million without coverage by 2026.
TIP: If the above didn’t make it clear, people tend to use the term “Single Payer” very loosely to express the general concept of “universal healthcare” (AKA access to essential healthcare for everybody). The reality is, there are many different ways universal healthcare can work, and many countries already have a form of universal healthcare that is working (generally a hybrid form of single payer that uses public and private methods; as noted). HealthCare Triage has done videos on many of the world’ universal healthcare system. See HealthCare Triage’s International Health Care Systems playlist or check out their videos below.
Unlike ObamaCare which has private and public insurance and private healthcare, a single payer system would generally have public insurance and private healthcare. With that in mind, a single payer system can be paired with a public healthcare delivery system, like it is with England’s NHI.TIP: As noted above, the ACA (ObamaCare) moved America toward universal healthcare via Medicaid expansion, cost assistance, and the mandate system. The mandate system is one of a few different universal healthcare systems. The problem with ours is that not getting coverage meant a fee, not a bare bones plan. ObamaCare didn’t offer insurance to everyone, so it wasn’t universal healthcare. TrumpCare offers insurance to even less, so it is even further away from universal healthcare.
TIP: Another type of universal coverage is called an all payer “rate setting” healthcare system (in which all third parties pay the same price for services at a given hospital; France and Maryland do this for example), meanwhile “a public option” is a single payer that people can opt-into by buying into it. There was supposed to be a public option in the ACA, but it was taken out by conservatives (conservative Democrats and Republicans) to ensure the ACA could pass. With that siad, progressive Democrats like Bernie and Obama helped ensure a waiver for state-level solutions was retained by the ACA. Learn more about the 1332 waiver.
TIP: People say single payer or universal healthcare can’t work in the U.S. because the other countries where it works well are smaller… but, we have 50 different states in a Union, and most are smaller than the countries where it is working. See: The Idea Universal HealthCare Can’t Work in the U.S. Due to Size is a Myth.
TIP: Our current system that rations care based on cost, excluding the poor to save dollars while burdening the middle class. One benefit of universal healthcare is that it doesn’t ration access to basic care based on cost. A benefit of the hybrid system is that non-essential care can still be rationed based on cost, thereby letting the market system work for non-essential care.
FACT: A “pure” single payer system eliminates private insurance and replaces it with a single fund, typically run by a single entity such as a government agency. Most countries haven’t implemented a “pure” single payer system and instead have retained some aspects of private insurance. Keep reading to understand different ways different types of single payer systems have been implemented around the world and how supplemental coverage, cost sharing, and tiered systems can remain in place in a single payer system.
Compare Canada’s Healthcare System to our healthcare system by watching this video and the next one (we’ll compare more systems below). Canada’s system is one of thirty-two different types of Universal HealthCare that range from socialized to the capitalist mandate-based systems. Canada’s system is working just fine, as are most of the other universal healthcare systems. The idea that single payer doesn’t work is essentially a myth.Single Payer, Medicare-for-All, Universal HealthCare, and the Related Semantics
Before we move onto answering specific questions about single payer, it is important to note that when people say they want “single payer” they may be being specific, but they may also just be expressing the desire to move toward a more comprehensive Universal Healthcare system.
Other terms used to describe types of single payer-like or universal healthcare systems include: a public option, national health care, and Medicare-for-all.
Each term has specific meaning, just as single payer means “a single public fund” specifically, but they all generally describe types of Universal Healthcare Systems or systems that seek to provide at least access to care for all, even if there is supplemental coverage, mandates, private coverage, etc.
So if you hear arguments for or against a specific term, make sure to inform people of the many different ways in which universal healthcare can work (and the many different ways single payer can work specifically).
TIP: The video below looks at why our current system is so expensive despite excluding tens of millions form coverage. The goal of single payer isn’t just to cover everybody, it is also to reduce costs!
Why is our healthcare so expensive? This video takes a look at that. Remember our problem is unique and complex to America, and the solution will be too. That’s true for the ACA, and it would be true for any healthcare funding or delivery system we put into place.TIP: See Bernie Sanders’ American Health Security Act, S. 1782 for an example of single payer legislation. In this case, it is a “Medicare-for-all system” with a “public network.” Also note, President Obama and Bernie Sanders had originally pushed for a public option. All these systems are allowed for under the ACA via a sec. 1332 waiver. So, repeal aside, if that provision remains, state-based systems are still possible.
What Would A Single Payer System Look Like In America?
A pure universal single payer health care system would be paid, in part, through taxes based on income replacing insurance premiums, copays, deductibles, etc. All plans would have the same benefits and networks. This would replace our multi-tiered system that rewards income with quality care.
That being said, the exact way single payer might be run in is flexible and could include a mix of public and private options like the Affordable Care Act, create a third public option in addition to Medicare and Medicaid, or simply create a Medicare-for-all system. These systems could retain supplemental insurance and cost sharing or not.
If we were to implement a single payer system in America, the way in which it was done would drastically change its effects. It’s unlikely that we would move from our current system to a pure universal healthcare system that didn’t include a supplemental aspect as it would require a more extensive overhaul of the current health insurance system.
What is the Difference between single payer and a public option? In simple terms, public option means an optional public fund (a fund people can opt into, generally by buying into it). This solution can exist alongside other health insurance and doesn’t haver to be the only option. This is one way to move toward a single payer while allowing the private market to compete. Another single payer option in the current system includes states using sec. 1332 waivers. Sanders, Obama, and Clinton, recently endorsed a public option as the next step in healthcare reform. See: Sanders Endorses Clinton, Clinton and Obama Endorse Public Option or see our page on ObamaCare and the public option.
Examples of Single Payer in America Today
We in America already have health insurance types that use a single fund, but the way delivery of care works differs depending on which type we are discussing.
Medicaid, Medicare, federal employee benefits, and state and local government benefits all use single funds, but use private delivery.
In Veterans Affairs and the military, we have a single fund and public delivery of care (VA recipients go to the VA for most care, for example).
Medicare only offers basic coverage as public insurance (Parts A and B) and let’s private insurers control the supplemental market (Parts C, D, and Medigap) making it an example of a mixed delivery system.
Each system can also use a mix of state and federal funding. Each system can also include taxes, regulations, and subsidization like with Medicare.
How Would Single Payer Affect HealthCare Spending?
A Single payer system would be expected to lower healthcare spending due to reduced administrative costs and improved bargaining power. We would expect less of a focus on profit, and more of a focus on care and prevention. Since all insurers would be under one roof (the entity that controls the fund), they would have tremendous buying power, which would help to curb the current health care crisis caused by skyrocketing health care costs. We could possibly maintain a healthier population requiring less treatment and spend more money on care and less on overhead.
On the other side of things, as mentioned above, the US already has a number of Government run “single payer” health care systems: Medicare, Medicaid, Veterans Affairs, military, federal employee benefits, state and local government benefits. That hasn’t stopped us from spending more per-capita on healthcare than any other nation on earth. What one could argue is that these systems have to compete with and operate in our current private market and operate with different budgets and restrictions, which could account for some of their shortcomings.
Would Single Payer Work in America?
Single Payer won’t magically fix our problems alone, but addressing the profit in health care funding, our current lack of bargaining power and the simplifying of coverage options would carry many benefits for the average American.
We know that single payer technically works in America because of the single payer systems we already have like Medicaid and Medicare, whether they currently work better than the private health insurance market and whether of not that would change depending upon how we implemented single payer is another more complex debate.
A single payer system would have to come with its own set of health care reforms that help ensure that the healthcare industry could still be as innovated and effective as it is today. Comparing what a single payer solution for America would be to other single payer systems or even to our single payer systems can only give us small clues as to what the actual outcome would be like. One of the best ways to look at how single payer would work is to look at previously proposed single payer legislation like the 2009 “Medicare-for-all” bill.
What is Medicare For All?
Medicare for all is a term used to describe a single payer system that essentially expands Medicare to everybody, but with some major differences. Despite the flexibility of single payer, the type of single payer discussed in America tends to focus on the 2009 bill The United States National Health Care Act, or the Expanded and Improved Medicare for All Act, (H.R. 676) which includes very specific ways in which single payer policies should be handled.
Under a Medicare-for-all type of single payer system, all Americans would be covered for all medically necessary services: doctors, hospitals, preventive care, long-term care, mental health services, reproductive health care, dental, vision, prescription drug, and medical supply costs. Patients would retain a free choice of doctor and hospital, and doctors would regain autonomy over patient care.
FACT: The term Medicare-for-all is often used interchangeably with single payer in America; however. it is actually a specific reference to a specific type of single payer system as defined by the 2009 bill The United States National Health Care Act and the Expanded and Improved Medicare for All Act (H.R. 676).
State or Federal Single Payer?
In 2017, states will be able to get a waiver to set up their own approved health care solutions, as long as they meet the standards of the Affordable Care Act. This will technically allow states to implement single payer systems on a state level, Vermont has already stated this is the direction they will take. Single payer systems are typically thought of something handled by the federal government, but in America it more likely that we will see single payer on a state level first.
The success of a state-based single payer program is likely to have an influence over whether or not we implement a single payer system as a country. “RomneyCare” was implemented in Massachusetts years before “ObamaCare” (which uses an almost identical framework) became “the law of the land.”
Different Types of Single Payer Systems Around the World
Different types of single payer systems can be found throughout the world, although most take a mixed approach. Popular examples of single payer systems include the UK, Canada, and Australia. Let’s take a basic look at these systems and how they differ from each other and ours.
Australia: Australia has had a Medicare for all system since 1984, which is publicly funded, but allows for a private option also at extra cost. The cost of the basic system is a 1.5% income tax levy. There is an exception for low-earners and an extra 1% tax for high earners.
In the U.S. our current system includes much higher taxes and the requirement for most of us to obtain private insurance as well.
Canada: Canada’s single payer system was set forth by the provisions of the Canada Health Act of 1984 works on a sliding scale based on income. Most people in a region have the same plan, with the same benefits. Since doctor payouts aren’t as high, it has led some doctors to seek employment in the US.
Our system is more expensive, but typically our higher-end private insurance can buy shorter wait times and higher end treatments. It does not buy less expensive medication. For instance, the comparatively low cost of Canadian drugs has led to many Americans using Canadian pharmacies.
UK: In the UK different countries have different systems with different mechanics. However, each system is paid for in a single payer fashion via taxation and is free at the point of need for the public. There are also private and employer-based options in the UK, although they account for a relatively small part of their health care system.
As with the other universal single payer systems, the UK provides a less expensive and technically a mixed market, approach to health care.
FACT: Single payer describes healthcare funding, not delivery. Universal healthcare can describe both funding and delivery. (Learn more about how single payer funding and how public healthcare delivery has worked in other countries).
Non-Single Payer Systems
There are few true single payer systems in the developed world like the ones discussed above. Most countries, like the US does now, rely on a large number of insurers.
Germany, for instance, has more than 150 “sickness funds.” The Swiss and Dutch health systems look a lot like ObamaCare’s health-insurance marketplaces. In France, about 90 percent of citizens have supplementary health insurance. Sweden has moved from a single payer system to one with private insurers. It is worth noting that all these countries pay vastly less for drugs, surgeries or doctor visits than Americans do.
ObamaCare can be a step toward single payer. In 2017 each state will be able to create unique solutions to the health care crisis, using the tools provided in the Affordable Care Act as a framework.Supplemental Options for Single Payer
In the US a single payer system might work like Medicaid, which is a one-size-fits-all solution to healthcare with no supplemental option, or it might work like Original Medicare, which can be paired with private supplemental insurance. There are choices and trade-offs. Retaining supplemental coverage means an easier transition from our current system, but adds complexity, bureaucracy, and retains our tiered system. It also allows for the continuation of our huge, and immensely profitable, health insurance companies. A system without supplemental options risks creating a sub-par health care system, compared to the care one can buy today. In most of the world, more money buys better medical care. A pure socialist system without supplemental options, which delivered effective care to everyone at the level we can provide to some today, would come at a huge price-tag, and most likely be unacceptable to most Americans.
Out-of-pocket Costs, Premiums, and Non-Essential Services
Possible universal healthcare could allow for a number of options. A single payer system could cover 100% of out of pocket costs, or it could simply offer everyone standard cost sharing. The same thing applies to premiums. These could work on a sliding scale based on income, like in Australia, or could be accessible to everyone. There is also a choice of covering all medical services or only essential services. If some services aren’t covered, but can still be obtained at a price, it might draw quality providers and manufacturers away from essential services focus them on pay-for-service care.
We have seen this happen in America in cosmetic surgery, for example.
Single Payer Versus ObamaCare
The difference between a single payer system and ObamaCare is that ObamaCare has both public and private insurance, with private care and some public care such as in the military system, while a single payer system has public insurance only with public and private care.
ObamaCare is a mixed-market approach to healthcare that embraces both public and private health care and health insurance and uses taxes, subsidies, and a mandate to obtain insurance to help keep uninsured rates low and sustain costs. Like a single payer system, it also works to address underlying health care costs, which are one of the major roots of our current health care crisis.
Let’s take a look at some differences between ObamaCare and a pure single payer system:
• Millions may remain under-insured or uninsured under the Affordable Care Act; it doesn’t guarantee coverage, it guarantees access to health insurance if one can afford it. Single payer guarantees coverage regardless of income.
• Insurers are allowed to limit benefits, medical networks, and care, and increase patients’ co-pays, deductibles and other out-of-pocket costs under the ACA. This is true despite new restrictions and regulations like the requirements for plans to provide minimum value and ten essential benefits. Benefits and doctors networks aren’t limited by insurers, and patient costs are replaced by taxes in a single payer system.
• In a true single payer system, no one needs to shop for health insurance. By avoiding under-buying and overbuying, we remove not only confusion but avoid people spending more or less than they need to (which can often lead to inadequate care). If the single payer system had supplemental insurance, as Medicare does now, this would be less true.
• Under our current system, the more you make, the better care you get. In theory, a pure single payer system would encourage us to ensure all care is good since we would all share the same benefits.
• A single payer system would allow for all-payer rate setting, a system in which insurers band together to negotiate rates collectively. Currently, each insurer and health care provider uses a chargemaster to negotiate prices. Since insurers negotiate rates for you, we don’t all pay equal prices for the same care under the current system. The for-profit spirit and lack of regulation behind this has contributed to the underlying health care cost in the US and the US health care crisis.
• In a single payer system we could reduce medically related bankruptcy due to people being underinsured or uninsured.
• In a single payer system there would be no fees for missing deadlines. For instance, if you miss your Medicare Part D enrollment, you could pay more for life, and if you miss open enrollment in the Health Insurance Marketplace, you can’t get coverage and pay a fee for not having coverage.
Single payer bill, H.R. 676 was introduced in 2003 and reintroduced in 2009. It focused implementing a universal single payer health care system in the US. Despite the significant support, the Affordable Care Act was eventually passed instead. Here are some differences between the ACA and the single payer bill.
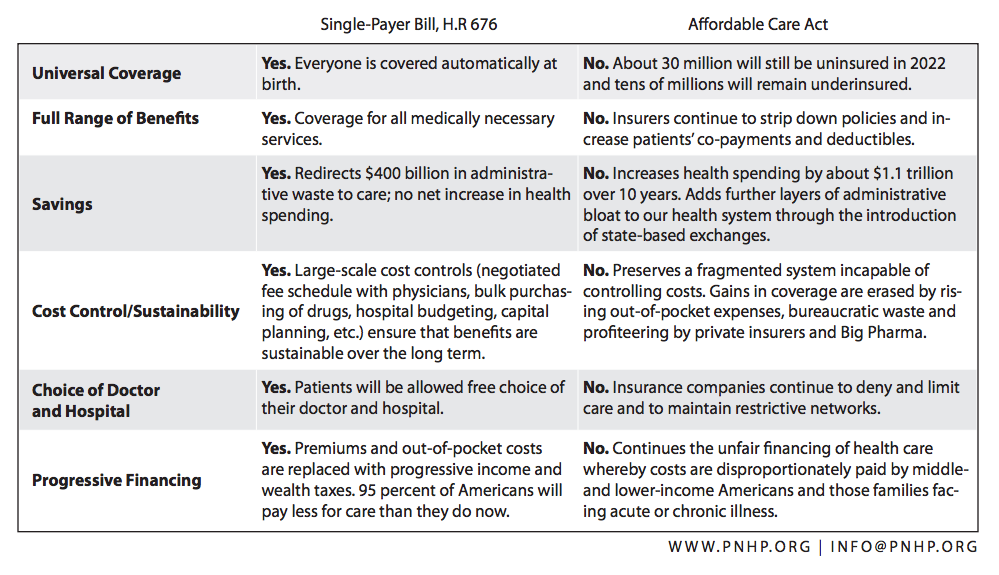
TIP: You’ll notice the above graphic mentioned price controls. Price controls are essential to any single payer plan. One problem with using government funds is a risk that it would distort the market. Smart price controls can help avoid market distortions. The goal would be to avoid anyone being undercut (we don’t want providers getting hurt, or patients, and we don’t want the government abusing its role for gains on that side either). Cost controls are vital and complex!
Is Single Payer Insurance Socialized Medicine?
The term “socialized medicine” tends to evoke a spirit of communism and can be a McCarthyistic buzzword. It doesn’t describe anything we are considering doing in America.
Socialized medicine implies, its buzzword status aside, a system in which doctors and hospitals work for and draw salaries from the government. Doctors in the Veterans Administration and the Armed Services are paid this way.
Single payer is more like Original Medicare and less like “socialized medicine.” With single payer doctors are in private practice and are paid on a fee-for-service basis from government funds. The government does not own or manage medical practices or hospitals.
The term socialized medicine is rarely used accurately and is instead often used as a buzz word to turn people away from progressive ideas.
Single Payer and Health Care Rationing
One of the points made against single payer insurance (and ObamaCare for that matter) is that it will lead to health care rationing and long wait times for appointments. While it is true that increased demand does have this effect, our pre-ObamaCare system and even our new system both already have healthcare rationing and wait times.
Before the Affordable Care Act, healthcare was rationed based on income and health status. Unless you could pay enough, you were restricted regarding benefits, care, doctors, wait times, treatments, etc. Post-ACA insurers and providers still ration care based on income (better plan, better coverage), although they can no longer ration care based on health status. If you think wait times can be bad for the Veterans Administration, the Armed Services, or Medicaid, you should see what the clinic wait times are for those without insurance or money.
In America, we outspend all other countries in health care spending and still ration care based on cost. Expanding coverage to the now 13.4% without insurance would add tens of millions of patients, but could potentially free up to an estimated $300 billion annually (3), This could be used to provide care, fund health care providers, and make other improvements to limit wait times and rationing.
Ultimately, it’s not necessarily the type of system we have that dictates rationing or wait times. Wait times boil down to the supply of doctors and medicines, versus demand from our numbers of patients and the amount of care they need. Unless we match supply and demand perfectly, healthcare will always have to be rationed, be it by wait times, referrals, care limits, or cost.
Does Single Payer Insurance Mean More Bureaucracy
The United States has arguably one of the most bureaucratic health care systems in the world. Over 31% of every health care dollar goes to paperwork, overhead, CEO salaries, profits, etc. Because the U.S. does not have a unified system that serves everyone and instead has thousands of different insurance plans, each with its marketing, paperwork, enrollment, premiums, and rules and regulations, our insurance system is both extremely complex and fragmented.
In America, Medicare operates with just 3% overhead, compared to 15% to 25% overhead at a typical HMO. Provincial single payer plans in Canada have an overhead of about 1%.
If you have ever tried to shop for a health plan, shop for health care, or contest a claim, you should know just how complex and bureaucratic health care already is. There is no question, signing up for Original Medicare, or Medicaid under the Affordable Care Act’s Medicaid expansion is relatively simple in most cases. What is complex is picking and choosing Private coverage options based on projected needs for care and projected income. This leads to over-buying or under-buying health insurance, not to mention the risk of incurring penalties for missed deadlines. While private insurance options may equate to profits for the health insurance industry and may be a great deal for some number of consumers, they lead to overspending in health care for Americans as a whole.
It is not necessary to have a huge bureaucracy to decide who gets care and who doesn’t when everyone is covered and has the same comprehensive benefits. With a universal health care system, we could potentially be able to cut our bureaucratic burden in half and save over $300 billion annually. (3)
Single Payer And Big Business
When we talk about a single payer system, we have to take into account the very real people and industries in the US who are tied to our current system. Many businesses and their employees depend on the nearly three-trillion-dollar, for-profit health care system, as do shareholders in these companies. We aren’t just talking about big-wigs and CEOs; we are talking about part-time nurses, ordinary hospital workers, and those in the hospital food service industry. These are people struggling to make living wages. Destroying an entire industry isn’t going to solve any healthcare crisis; our problems are bigger than CEO salaries and shareholder profits. A true solution must take all of this into account, just as the Affordable Care Act Does. That being said…
In 2009, Forbes ranked health insurance as the 35th most profitable industry. That sounds high, and it is, but it doesn’t even begin to compare to other health care industries. The pharmaceutical industry was in third place, with a 19.9 percent return, and the medical products and equipment industry was right behind it, with a 16.3 percent return. Meanwhile, doctors average in the top 5% of earners, and specialists often are in the top 1%.
In other words, there is a huge amount of money being spent and made in health care and “pulling the plug” overnight would have a catastrophic effect. Luckily a single payer system doesn’t just do away with private health care (remember it makes insurance public, not healthcare). It does, however, give a lot more power to the consumer and puts pressure on the health care industry to start running smarter so we can start addressing the underlying issue of health care costs.
Current Health Care Costs
Data gathered by the International Federation of Health Plans show that an MRI costs, on average, $1,121 in the United States and $363 in France. An appendectomy costs $13,851 in the United States and $4,782 in Switzerland. A birth by cesarean section costs $3,676 in the United States and $606 in Canada. A bottle of Nexium — a common acid-reflux drug — costs $202 in the United States and $32 in Britain. (Related: “Why an MRI costs $1,080 in America and $280 in France“.) (3)
Why does health care cost so much more in the US? Is it better? Unfortunately, that is not the case. While we do some things better in healthcare, we don’t do simple things like Aspirin, Nexium, or MRIs better. The issue here has more to do with the deals made between insurers and healthcare providers.
Why Does America’s Health Care System Cost More?
In most countries, people use the same amount of Medical services but pay much less. This is true regardless of whether they use a single payer system or not. Why? Because in most countries the government sets prices for health-care services and products. Insurers in Switzerland don’t negotiate drug prizes with Pfizer. The Swiss government simply sets its drug prices and lets Pfizer decide whether to sell in Switzerland — or not. In short, it’s not simply the type of funding that dictates our healthcare prices; it’s how we come about the base costs. (3)
How Will We Keep Drug Prices Under Control?
When all patients are under one system, the payer wields a lot of clout. The VA gets a 40% discount on drugs because of its buying power. This “single” buying power is the main reason why other countries’ drug prices are lower than ours. This also explains the drug industry’s staunch opposition to single payer national health insurance. The medical device industry is also complicit in this issue. The ACA created a 10% tax on both of these industries as a response. (2)
Why Shouldn’t We Let People Buy Better Health Care if They Can Afford it?
Whenever we allow the wealthy to buy better care or jump the queue, health care for the rest of us suffers. If the wealthy are forced to rely on the same health system as the poor, they will use their political power to assure that the health system is well funded. Conversely, programs for the poor become poor programs. For instance, because Medicaid doesn’t serve the wealthy, the payment rates are low, and many physicians refuse to see Medicaid patients. Calls to improve Medicaid fall on deaf ears because the beneficiaries are not considered politically important. Moreover, when the wealthy jump the queue, it results in longer waits for others. Studies in New Zealand and Canada show that the growth of private care in parallel to the public system usually results in lengthening waits. Additionally, allowing the development of a parallel, private system for the wealthy means the creation of a permanent lobby for underfunding public care. Such underfunding increases the demand for private care. (2)
Does Single Payer Work?
Our health care system was in crisis before the Affordable Care Act. While the ACA took a lot of aspects of a single payer system and combined them with our current insurance industry-driven healthcare system. This has staved off some of the crisis but has by no means solved it. A single payer health care approach has worked for other countries, and it, of course, could work for us. However, a single payer system on its own won’t offer the solutions our country needs. The focus of the ACA and future healthcare reform can’t just be about how we get health insurance. It has to be about what insurers, whether they are one payer or many, actually pay for care. As long as we have a system where you can be charged $75 for an aspirin at the hospital, no amount of insurance reform is going to solve the issue.
Why Don’t We Address Medical Costs?
The Affordable Care Act does a lot to “curb health care spending” and includes provisions that address big issues mentioned above like doctor payments, medical device taxes, taxes on the pharmaceutical industry, provisions that make insurers spend more profits on care, and more. Unfortunately, for all the law does to address these issues, it still leaves a for-profit system in place that decides the medical costs in the US. In our current system, the government holds the power to negotiate some prices but isn’t allowed to exercise it to an effective extent, while the insurers are experts at running the industry. The solution must be developed by the public, insurance industry, and Government compromising to reform a health care industry that has become the root of unaffordable health care in the US. Luckily this idea has a name “all-payer rate setting.”
All-Payer Rate Setting
All-payer rate setting is a system in which insurers band together to negotiate rates collectively. We the people could shift our current “ObamaCare” based system to a single payer system with all-payer rate setting. This one move could take power away from for-profit health care providers and put it in the hands of the American people.
Health-care providers — not insurers alone — have a great deal of power in the US system. As a result, they have the most to lose if health-care prices fall. But, as is often the case, political power flows in part from profitability. So politicians who routinely rail against for-profit insurers are scared to criticize — much less legislate against — for-profit hospitals, doctors or device manufacturers (though drug companies come in for a drubbing now and then). These are the people who work every day to save our lives, even if they make us pay dearly for the privilege. (3)
Is the Insurance Industry Good?
Insurers aren’t good or bad. They preform an important function in the health care sector. Regardless of how we move forward, we will need the insurance industry. Remember single payer plans opt for a public insurance industry, not the elimination of insurers.
Currently private insurance overhead is about 500 billion a year; a single payer system with a 2% overhead, as with Medicaid, Medicare, etc. It could potentially cost 50 billion, saving 450 billion, 80% of our entire deficit to change the system. In addition, insurers are fragmented and their lack of group buying power means they each end up paying higher prices for medical services and pass those costs onto us with higher premiums and greater out of pocket costs. The better we can structure our insurance industry, the better we can deal with the economic aspect of the health care crisis. (3)
The Dangers of Single Payer Insurance
One can argue there are some dangers to single -payer healthcare. Most have already been addressed above, but we will summarize them before we close so we can ensure we are giving weight to both sides of the ongoing argument for and against single -payer insurance being potentially used in America:
• It would be like Medicaid. Medicaid can be said to provide limited care. Medicare has been known to provide good care, although this may well change now that the compensation scale for medical providers has been adjusted downward. The quality of any system depends partially on rates paid to providers. The goal is to have good care for all. The aim is to use group buying power (and group voting power) to ensure that care is up to par. Achieving this may mean we sacrifice some potential reduction in healthcare spending for quality of care.
• Rationed Care. If everyone has equal access to care, then it increases wait times. While this might be true at first, demand tends to rise first, and then supply meets it. If we keep healthcare providers’ rates high enough, it will incentivize jobs. That means more workers are stepping up to meet the demand. If we keep care private, only insurance would be changing. Remember also that we already ration care in America based on income. Under the ACA, we saw an increase in demand and that led to longer wait times. This is why that same law creates incentives for new healthcare workers. A single payer system would be likely to do the same thing.
• Research, Innovation, and Development are hampered. Medicare is currently the most profitable field in healthcare and companies are constantly innovating in the Medicare market. Companies innovate for Government contracts. Again healthcare remains private, so businesses continue to compete. Only insurance is public under a single payer system. Will big business drug maker X really stop innovating just because they only have to make one deal with everyone instead of a bunch of little deals with a number of entities?
• Single Payer systems won’t save money and may be more expensive. This argument is made well by Bloomberg View.
Resources
The following sources were used to present an unbiased look at a single payer system in America.
1. Wikipedia
2. PNHP
The Future of Single Payer
For today the Affordable Care Act is the law of the land. After a century of health care reform attempts we are better off than we have ever been. Costs are decreasing, and the insured rate is going up, but we have more work to do. Come 2017 states may begin to implement single payer under the ACA, and this could very well lead to all-payer rate setting in those states too. We could even have the single payer debate sooner depending upon what happens with the 2016 Presidential candidates.
As insurers move into a post-ACA mindset and work closer with the people and our government, we may be able to address some of the deeper underlying issues of health care costs. As long as the ACA can stand un-repealed, it may have the room to truly address the healthcare crisis.
- the Human Development Index – official list
Author: Thomas DeMichele
Thomas DeMichele is the head writer and founder of ObamaCareFacts.com, FactsOnMedicare.com, and other websites. He has been in the health insurance and healthcare information field since 2012. ObamaCareFacts.com is a...
Thomas DeMichele's Full Bio